
The Complete Nervous System Guide for Anxiety
By Katie Hargreaves, LCSW, LCAS | Somatic Therapist | Hollywood, CA & North Carolina
Last updated: June 5, 2026
“Anxiety is not a thinking problem. It's a survival problem. And your nervous system is the one trying to solve it."


1. What your nervous system actually is — and why it runs the show
Let's start here, because most explanations of the nervous system are either so technical they lose you, or so vague they don't actually tell you anything useful.
Your nervous system is the biological infrastructure that keeps you alive. It's not just your brain — it's the entire communication network between your brain, your body, and your environment. It's running 24 hours a day, processing thousands of signals, and making constant decisions about what's safe and what isn't — mostly without ever consulting you.
That last part is important. The parts of your nervous system most relevant to anxiety operate below conscious awareness. They're faster than thought. By the time you notice you're anxious — the tight chest, the racing heart, the thought spiral — your nervous system has already been in an activated state for several seconds. You didn't decide to feel anxious. Your nervous system decided for you.
This is not a flaw. This is the whole point. If your threat-response had to wait for you to consciously evaluate every situation, you'd be terrible at surviving. The speed and automation of the stress response is what kept humans alive for hundreds of thousands of years.
The problem isn't that the system exists. The problem is when it gets stuck — when it keeps responding to current situations with patterns it learned in very different circumstances. When your nervous system learned that the world wasn't safe, it filed that lesson away and kept applying it. Even after the circumstances changed. Even after you grew up, moved away, built a different life. Even after you understood, intellectually, exactly what was happening.
Your nervous system doesn't update through understanding. It updates through experience. And that's the whole story of why anxiety is so resistant to the things that should work — and why the things that actually work are so different from what most people try.
Here's what I want you to take from this section: you are not anxious because something is wrong with you. You are anxious because your nervous system is doing its job — just with outdated information. The work we're talking about in this guide is not about fixing yourself. It's about giving your nervous system new data.
If you want to understand the specific mechanism of how anxiety gets stored in the body, read: How Your Nervous System Creates Anxiety — And What Somatic Therapy Does About It.
If you're ready to work with someone on this directly, somatic therapy in North Carolina and somatic therapy in Hollywood are both available virtually.
2. The three states your nervous system lives in
This is where it gets genuinely interesting — and where most people have a moment of recognition that makes everything click.
Stephen Porges, a neuroscientist and psychiatrist who spent decades studying the autonomic nervous system, developed what he called Polyvagal Theory. It's become one of the most important frameworks in trauma and anxiety treatment in the last 30 years — and once you understand it, you will never think about anxiety, shutdown, or that "wired but tired" feeling the same way again.
Porges' theory proposes that the autonomic nervous system has three distinct states, organized in a hierarchy. They evolved in sequence over millions of years, with the newest, most sophisticated one on top. When things get hard enough, your system moves down the hierarchy — from the newest response to older, more primitive ones.
Here they are, from newest to most ancient:
State 1: Ventral vagal — safety, connection, actual presence
This is your "I'm okay" state. When your nervous system is in ventral vagal activation, you feel:
Genuinely calm — not forced, not performed, but actually settled. Present in your body. Able to connect with other people without it costing you enormous energy. Curious rather than hypervigilant. Able to sit with uncertainty without immediately needing to resolve it. Able to rest and actually feel restored by it.
This is where your best thinking happens. Where creativity lives. Where real intimacy is possible. Where you can disagree with someone without your heart rate going up.
For a lot of people reading this guide — people who have been anxious for a long time — ventral vagal feels like a foreign country. Like something other people get to live in. You might recognize it in brief moments: a few hours on a really good vacation, the first ten minutes after a workout, a rare night of genuinely deep sleep. And then it's gone.
State 2: Sympathetic activation — fight or flight
When your nervous system detects threat, it mobilizes. Cortisol and adrenaline flood your system. Heart rate increases. Blood moves to large muscle groups and away from digestion. Your vision narrows. Your thinking becomes faster and more binary.
This is fight or flight — and it is an extraordinarily effective survival response. If there is a real physical threat, this state will help you respond to it faster and more powerfully than you could from a relaxed baseline.
The issue, as you probably know, is that your nervous system activates this state in response to threats that are not actually physical — performance pressure, relationship conflict, an ambiguous email from your boss, the thought of a difficult conversation you need to have, the sensation of having too much to do. Your body's threat-response doesn't distinguish between a predator and a passive-aggressive text message. It responds to perceived threat, full stop.
In chronic anxiety, your sympathetic system is partially activated most of the time. It never fully settled back to baseline. That's the background hum — the persistent sense that something is wrong, or is about to go wrong, even when your life is technically fine.
Sympathetic activation that runs chronically produces what you probably recognize as the physical experience of anxiety: muscle tension that lives in your shoulders and jaw. The gut that's always a little off. The heart that beats just a little too fast. The breath that stays shallow even when you're not stressed. The sleep that doesn't fully restore you because you're never fully off alert.
State 3: Dorsal vagal — shutdown, freeze, and collapse
This is the oldest part of the hierarchy — the most primitive survival response. When a threat feels completely overwhelming and fight or flight isn't possible or hasn't worked, the nervous system can shift into dorsal vagal shutdown.
This state is often misunderstood as "relaxation" because it involves a decrease in activation. It's not. It's collapse. Dissociation. Numbness. The inability to feel much of anything. The flatness. The "I know I should care about this but I can't make myself" experience. Fatigue that doesn't respond to rest. Difficulty being present in your own life.
In evolutionary terms, this was designed for situations where survival required stillness — playing dead, becoming invisible. For animals, it often precedes or follows traumatic injury. For humans, it shows up as the nervous system's response to overwhelm that has gone on long enough, or has been profound enough, that the system essentially went offline.
A lot of people reading this will recognize the dorsal vagal state from burnout. From depression that sits on top of anxiety. From the way chronic stress eventually stops feeling like anxiety and starts feeling like nothing.
The nervous system isn't a light switch. It's a volume dial. And most people with anxiety have theirs stuck between 6 and 8 on sympathetic, with occasional drops into dorsal shutdown. Ventral vagal — the actual "I'm okay" state — feels like it's on a different channel entirely.

Here's the thing most people don't know, and that I think is genuinely life-changing once it lands: these states are not chosen. They're not character flaws. They are physiological responses. You cannot willpower your way from sympathetic activation into ventral vagal. You cannot think yourself calm. Not because you're not trying hard enough — but because the thinking brain is not in charge of the state your nervous system is in.
What you can do is learn to work with the nervous system directly. That's what this entire guide is about. For a full breakdown of polyvagal theory and what it means for anxiety treatment, read: Polyvagal Theory Explained.
3. How anxiety gets stuck — and why it stays
Here's a question I get asked constantly, in various forms: "I know why I'm anxious. I've dealt with the thing that caused it. Why is it still here?"
This is the question that most traditional therapy doesn't have a satisfying answer to. And understanding it is what changes everything.
Peter Levine, a biophysicist and psychologist who spent decades studying trauma and stress responses in animals and humans, observed something important: in animals, the stress response has a completion sequence. The gazelle gets chased by the lion, escapes, and then — before going back to grazing — shakes, trembles, and moves through a full discharge of the mobilized energy. After the completion, the nervous system returns to baseline. The gazelle doesn't have PTSD.
Humans often don't get to complete the sequence.
When threat activates the fight-or-flight response and we can't run or fight — because it's a social threat, because we're in a meeting, because we're a child and the threat is in our own home, because freezing felt safer — the mobilized energy doesn't discharge. It stays in the body. The nervous system remains in a partial state of activation because, as far as it's concerned, the threat was never fully resolved.
Over time, this undischarged activation becomes the nervous system's new normal. The threat response stays partially online. The body keeps scanning for danger. The stress hormones keep running at a lower but continuous level. And when new situations arise that have even a vague resemblance to old threatening ones, the nervous system overreacts — because it's already starting from an elevated baseline.
This is why anxiety can persist long after the original circumstances have changed. Your nervous system isn't responding to your current life. It's responding to the accumulated history of unresolved activations — and applying that history to everything that comes after.
This is also why insight alone doesn't resolve it. Understanding that your anxiety comes from your childhood, or from a difficult relationship, or from years of high-pressure work — that understanding is real and valuable. But it's happening in the prefrontal cortex. The activation is stored subcortically. The two systems aren't well-connected enough for one to simply overwrite the other.
The prefrontal cortex — the thinking, reasoning, insight-having brain — goes partially offline under threat activation. This is well-documented in neuroscience. It's one of the reasons that in moments of high anxiety, all the things you know about your anxiety become temporarily unavailable. Your nervous system has redirected resources away from higher-order thinking and toward survival responses. You can't think your way calm because the thinking part of your brain is not in charge during activation.
In your body:
You carry tension in your shoulders, your neck, your jaw — constantly, not just when stressed.
You've stopped noticing it because it's been there so long.
Your digestion is never quite right. You get sick more than you feel like you should.
Your sleep is technically fine but you never wake up feeling restored. Your heart rate is slightly elevated even at rest.
You hold your breath without realizing it, or breathe in a way that's shallow and restricted.
You startle easily. Loud noises, unexpected touches, sudden changes — your body reacts before your brain does.
In your thinking:
The loop never stops. You finish one thing and your mind is already on the next three.
You replay conversations — not because you're processing them, but because your threat-detection system is reviewing them for evidence of danger.
Your decision-making takes longer than it should because every option gets threat-assessed.
You catastrophize easily — not because you're a pessimist, but because your nervous system's job is to anticipate the worst-case scenario so you're prepared for it.
"Your nervous system isn't responding to your current life. It's responding to the accumulated history of unresolved activations."

So what actually updates the nervous system?
New experience. Specifically, the experience of activation followed by resolution — going into a stress response and coming back out of it safely, repeatedly, until the nervous system learns that activation doesn't have to become catastrophe.
This is what somatic therapy is designed to create. Not through analysis, not through insight, but through direct, carefully titrated work with the physiological states themselves. We create new experiences in the nervous system. We help it complete what was interrupted. We give it evidence — not arguments, but actual felt evidence — that safety is possible.
Want to understand more about how somatic therapy creates this kind of change? Read: Somatic Therapy in Los Angeles | Somatic Therapy in North Carolina
4. The Window of Tolerance — Your Anxiety's Actual Address
This is one of the most practically useful concepts in nervous system work, and once you understand it you'll start seeing it everywhere.
Daniel Siegel, a clinical professor of psychiatry at UCLA, developed the concept of the window of tolerance — the zone of arousal in which the nervous system can function optimally. Not shut down. Not flooded. Processing.
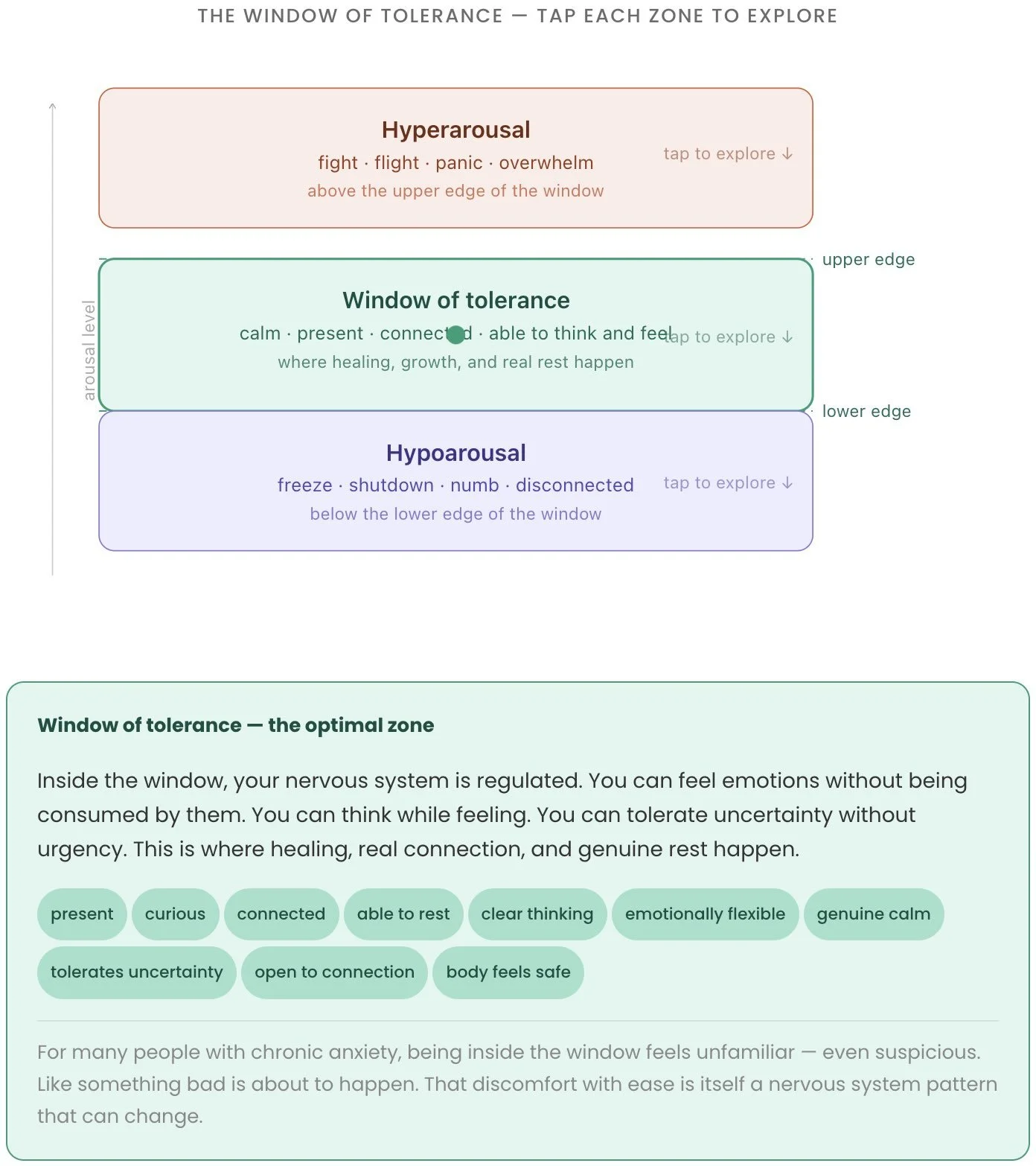
Think of it as a channel with two edges:
The upper edge is the threshold into hyperarousal — fight-or-flight territory. When you're pushed past this edge, you feel overwhelmed, flooded, reactive, panicky, unable to think clearly. Anxiety attacks live here. So does rage. So does the desperate overthinking that happens in the middle of the night.
The lower edge is the threshold into hypoarousal — dorsal vagal shutdown. When you drop below this edge, you feel numb, flat, disconnected, unable to feel or access emotion, exhausted beyond what rest can touch.
Inside the window: you can feel activated without being overwhelmed. You can access emotion without being consumed by it. You can think while feeling. You can tolerate uncertainty. You can be present.
Here's the problem for people with chronic anxiety: their window is narrow. Often very narrow. The slightest provocation — a tense email, a perceived slight, an unexpected change in plans — tips them above the upper edge. And after years of living in hyperarousal, the bottom drops out into shutdown. The cycle between flooded and numb becomes the emotional weather system.
The goal of nervous system work is to widen this window. Not to prevent all activation — activation is healthy and normal, and the goal is never a flatlined emotional life. The goal is to have enough range that you can move through activation without it taking over, and return to baseline without crashing into shutdown.
How does the window get narrow in the first place? A combination of things:
Early experiences where the environment was unpredictable, overwhelming, or unsafe — the nervous system learned to be hypervigilant because vigilance was actually adaptive. The window narrowed as a survival strategy.
Chronic stress that never fully resolved — the nervous system stayed partially activated for so long that the upper edge of the window dropped and the baseline shifted upward.
Trauma — both acute and developmental — that involved activation without resolution. The incomplete stress responses we talked about in the last section. Each one that didn't complete made the window a little smaller.
Lack of co-regulation — not having consistent access to calm, regulated nervous systems around you. Co-regulation is how nervous systems learn to regulate; if you grew up without reliable co-regulation, your nervous system had to do it alone, which is much harder and less effective.
Your window of tolerance is not fixed. It's not your personality. It's a learned physiological pattern — and learned patterns can be changed. Widening the window is literally what nervous system therapy is doing.
5. Why your body holds what your mind has already processed
This section is for the people who've done years of therapy, who have genuine insight, who understand exactly where their anxiety came from — and who are still anxious.
You are not failing at healing. You are experiencing the gap between cognitive processing and somatic processing — and it's one of the most important distinctions in all of mental health treatment.
Bessel van der Kolk, a psychiatrist and trauma researcher who spent decades at Boston University School of Medicine and Harvard, has probably contributed more to the mainstream understanding of this gap than anyone else. His research demonstrated, repeatedly and across large samples, that trauma is encoded differently from ordinary memory.
Ordinary memories are processed through the hippocampus and stored as narrative — a story with a beginning, middle, and end, filed in the past tense. "That happened then. It is over now."
Traumatic memory — and the memory of chronic threat — is encoded subcortically, in the body. In the amygdala's threat-response patterns. In the brainstem's survival reflexes. In the muscular holding patterns and postural habits that developed as protective responses. In the way your gut responds before your brain does. In the breath that stays shallow without your permission.
This is why you can know something is in the past and still have your body respond as if it isn't. The hippocampus knows it's over. The amygdala hasn't gotten the update. And the amygdala is faster.
Van der Kolk's phrase — the body keeps the score — became the title of his most famous book because it is simply, precisely true. The body is keeping track of everything that the mind has processed, filed away, and moved on from. The unfinished business isn't in your thoughts. It's in your tissue.
What this means in practice
It means that traditional talk therapy — as valuable as it is for building insight, narrative coherence, and relational skills — has a ceiling for this specific problem. You can narrate your trauma in perfect detail and your body can still respond with the same activation it always has, because narration doesn't update subcortical encoding.
It means that the people who feel "stuck" in therapy — who understand everything and still feel the same — aren't doing something wrong. They've reached the ceiling of what cognitive processing alone can accomplish. The next layer of work is physiological.
It means that somatic approaches — working directly with body sensation, completing interrupted stress responses, building new physiological experiences of safety — are not alternative or fringe. They are addressing the actual location of the problem.
This is what van der Kolk's research showed. This is what Levine's Somatic Experiencing model was built around. This is what Polyvagal Theory explains. This isn't a niche perspective in trauma treatment anymore — it's becoming the consensus.
A note on this for the skeptics
I know some of you reading this are scientists, clinicians, researchers. You've been trained to be appropriately skeptical of anything that sounds like it's explaining everything with one theory.
Fair. I'm skeptical too, honestly.
What I'd say is this: the claim isn't that somatic approaches explain everything or that cognitive approaches are useless. The claim is more modest and, I think, well-supported: for anxiety that persists after cognitive processing, body-based interventions address a dimension of the problem that cognitive interventions don't reach. That's it. That's the clinical argument, and it holds up.
The neuroscience behind it — subcortical encoding of threat memory, the relative disconnection between the prefrontal cortex and the amygdala under activation, the role of the autonomic nervous system in generating anxiety symptoms — is not controversial. The specific mechanisms of how somatic interventions change these patterns are still being studied. But the evidence that they do is strong.
For the full clinical breakdown of the research: Somatic Therapy North Carolina — the evidence base section
Key Researchers in Somatics
Bessel van der Kolk, MD
Boston University School of Medicine
The Body Keeps the Score · Trauma encoding
Demonstrated through decades of research that trauma is encoded subcortically — in the body's stress responses, not just in narrative memory.
Stephen Porges, PhD
University of North Carolina
Polyvagal Theory · Neuroception
Developed Polyvagal Theory, which describes how the autonomic nervous system operates in three hierarchical states — ventral vagal, sympathetic, and dorsal vagal.
Peter Levine, PhD
Biophysics & Psychology
Somatic Experiencing · Stress completion
Observed that animals discharge stress responses naturally after threat, while humans often suppress this process — leaving activation stored in the nervous system.
Daniel Siegel, MD
UCLA School of Medicine
Window of tolerance · Interpersonal neurobiology
Developed the concept of the window of tolerance — the zone of arousal in which the nervous system can process experience without flooding or shutting down.

Recognizing yourself in this? If anxiety has stayed in your body even after you've processed it cognitively, that's the clearest signal that somatic work is what's next.
I work with clients in California and throughout North Carolina. The consult is free, 15 minutes, no intake form required.

6. What nervous system dysregulation actually looks like day to day
Let's get concrete. Because "nervous system dysregulation" sounds like something that happens to other people — people who've been through serious trauma, people whose anxiety is visible and disabling.
Here's the truth: most of the people I work with don't look dysregulated from the outside. They look like the most capable person in the room. Dysregulation doesn't always look like falling apart. For a lot of people — especially high-achievers, especially people who learned early that holding it together was required — it looks like this:
If you're reading this list and checking boxes, I want you to hear this clearly: this is not your personality. This is your nervous system doing what it learned to do. And it can change.
The high-achiever presentation specifically
There's a particular flavor of dysregulation that shows up in high-achieving, high-functioning people — in the people who are excellent at their jobs, who produce and deliver and lead and hold things together — and I want to name it separately because it's so often missed.
In high-achievers, chronic sympathetic activation often looks like ambition. The inability to stop working looks like dedication. The hypervigilance looks like attention to detail. The perfectionism looks like high standards. The social hyperawareness looks like emotional intelligence.
And all of those things may genuinely be true at the same time. You may be ambitious, dedicated, detail-oriented, high-standard, and emotionally intelligent. And your nervous system may be using all of those qualities as vehicles for a threat response that never turned off.
The tell — the thing that distinguishes dysregulation from genuine high performance — is whether you can choose to stop. Whether rest is actually available to you. Whether you can sit in a moment of ease without the pull to fill it with something productive. Whether the driver of your output is desire and engagement, or whether it's the quiet terror of what happens if you slow down.
Most people who are running on dysregulation can't answer that last question clearly, because the pattern has been present so long it's become invisible. They can't see the threat response driving their ambition because they've never experienced it operating without it.
The post on signs your nervous system is stuck in fight or flight covers every physical, emotional, and behavioral signal in detail. For more about this type of dysregulation check out: High-Functioning Anxiety in Los Angeles: Why Success Doesn't Make It Stop
In your emotions:
You feel things intensely but have a hard time letting them move through you — they either flood everything or get suppressed immediately.
Your emotional range has narrowed over time. What used to bring genuine joy now brings a muted version of it.
Rest feels vaguely wrong, like you're getting away with something.
You feel guilty when you're not productive.
In your relationships:
You're hypertuned to other people's emotional states — you know when someone is slightly off before they say anything, and your system immediately starts scanning for what it might mean about you.
Conflict sends your nervous system into high alert even when it's minor.
Distance or silence from people you care about activates the same threat response as actual danger.
You give a lot and find it hard to receive.
In your energy:
You're exhausted, but you can't stop. The tiredness is deep and doesn't respond to rest, because you're not tired in the way that sleep fixes — you're running on a depleted nervous system, and that's a different kind of tired.
On better days you feel okay, almost fine. On harder days it tips into a flatness that scares you a little.
7. The difference between regulation and suppression — and why it matters
This one gets confused constantly, and the confusion is worth clearing up because it changes what you're aiming for.
Suppression is pushing activation down. Breathing through it. Talking yourself out of it. Distracting yourself. Staying busy enough that you don't have to feel it. Managing the symptoms so they don't interfere with your functioning. Most traditional coping strategies — and many therapeutic approaches — are, at their core, forms of sophisticated suppression.
Suppression works, up to a point. It's not nothing. It's what gets you through the day, through the meeting, through the hard conversation. But it has a cost: it keeps the activation stored in the body. The thing you breathed through didn't resolve — it was put back in the drawer. The drawer fills up over time.
Regulation is something different. Regulation means the nervous system moves through a state and returns to baseline. The activation completes. The stress response runs its course. The energy that was mobilized discharges. The system settles — not because you pushed it down, but because it actually finished.
The distinction matters enormously for treatment, because the goal of nervous system work is not to get better at suppression. It's to build genuine regulatory capacity — the ability to experience activation, move through it, and return to baseline without it destroying you or requiring enormous effortful management.
Here's why this is more than a theoretical distinction: people who have gotten very good at suppression often feel like they're coping fine — until they're not. The person who has managed their anxiety successfully for twenty years through sheer force of effortful self-management, and who suddenly can't, isn't experiencing a new problem. They're experiencing the accumulated weight of two decades of stored activation finally exceeding the capacity of the drawer.
Genuine regulation — the kind that comes from somatic work, from actually completing stress responses rather than managing them — builds capacity. Each time the nervous system moves through activation and settles, the window of tolerance widens slightly. The system learns that activation isn't permanent. It learns that it can return to safety. Over time, the regulatory capacity becomes less effortful and more automatic.
What regulation actually feels like
This is worth describing because for people who have been in chronic sympathetic activation for a long time, genuine regulation can be unfamiliar enough to feel wrong at first.
Real regulation doesn't feel like forcing calm. It's not the stiff, performed relaxation of someone who has decided to be fine. It's softer than that. It often arrives as a kind of settling — a heaviness in the limbs, a deepening of the breath that happens without effort, a warmth or tingling in the hands or feet as blood flow normalizes, a slight sense of the room expanding.
Some clients describe it as feeling their body for the first time in a long time. Others describe it as realizing they'd been bracing and finally being able to stop. It can feel vulnerable — and for people whose nervous systems learned that relaxation was dangerous, the first experiences of genuine regulation can actually trigger the threat response. (Which is why working with a skilled clinician matters: the titration has to be precise enough that the window can expand without triggering a defensive response.)
The more often the nervous system experiences this return to baseline, the more familiar and accessible it becomes. This is not about achieving a constant state of zen. It's about making safety available as an actual, felt option — not just a concept.


8. How somatic therapy works with the nervous system
I'm going to get specific here, because the word "somatic" gets thrown around a lot and deserves to be unpacked with more precision than it usually gets.
Somatic therapy is not a single technique. It's a framework — a set of approaches that share the common feature of treating the body's physiological state as a primary site of therapeutic intervention rather than an afterthought. Within that framework there are several distinct models, each with their own theory of change and clinical techniques.
Here's what I draw from in my practice, and why:
Somatic Experiencing (Peter Levine)
SE is built around the completion model I described in section three. The core idea: trauma and anxiety result from incomplete defensive responses, and healing happens when the nervous system gets to finish what it started — in small, carefully titrated doses.
In SE, the therapist tracks the client's physiological state closely — watching breath, color, muscle tone, movement impulses — and uses that information to guide the pacing of the work. We approach difficult material and then pendulate back to resource — moving between activation and settling, activation and settling, slowly building the nervous system's capacity to process without flooding.
The goal is not catharsis. You're not trying to have a big emotional release. You're trying to help the nervous system complete the procedural sequences that got interrupted. That looks quiet from the outside. Inside, it can feel like things slowly shifting.
Polyvagal-informed therapy (Stephen Porges)
Polyvagal Theory gives us the map — the three-state model I described in section two — and the understanding that the therapeutic relationship itself is a regulatory resource. Porges' concept of neuroception describes how the nervous system continuously scans the environment for cues of safety or danger, and how the cues it picks up from other nervous systems are among the most powerful.
This means the therapeutic relationship isn't just a context for the work — it's part of the mechanism. A regulated therapist, genuinely present and attuned, provides a co-regulatory resource that helps the client's nervous system access states of safety it might not be able to reach alone. This is why I'm intentional about my own regulation — about keeping my caseload manageable, about not seeing clients back-to-back, about doing my own work. A dysregulated therapist can't provide this.
In practice, polyvagal-informed therapy involves paying close attention to which state the client is in, offering cues of safety (tone of voice, facial expression, pacing, breath), and working to support ventral vagal access before moving into processing.
Internal Family Systems (Dick Schwartz)
IFS is a parts-based model — it works with the understanding that the psyche is organized into distinct parts, each of which developed in response to a specific need or experience. The parts most relevant to anxiety are often protectors — parts that took on the job of managing threat and keeping the person safe, often at significant personal cost.
The perfectionism that drives you past exhaustion. The hypervigilance that scans every social situation for danger. The part that can't stop working. The inner critic that tries to prevent failure by attacking you preemptively. These are all parts doing what they learned to do — and they respond very differently to being understood and appreciated than they do to being told to stop.
IFS work doesn't fight with the anxious parts. It gets curious about them. What were they protecting against? What do they need to know to be able to relax? When a protective part of the system feels genuinely seen and understood — not steamrolled, not bypassed — it often loosens its grip voluntarily.
Combined with somatic work, IFS is particularly powerful because we can work with parts at both the cognitive and physiological level — understanding the story and shifting the body state simultaneously.

What a session actually looks like
I want to demystify this because it sounds more esoteric than it is.
A 60-minute session might look something like this:
We start by checking in — not as a formality, but as clinical information. Where are you right now? What's your body doing? We're orienting to your current state before deciding what to work with.
If there's something present — an activation, a tension, a feeling that's sitting in the body — we turn toward it rather than away from it. Slowly. We notice where it lives physically. We get curious about it. We don't analyze it — we sense it.
As we work, I'm tracking your responses carefully. Breath changes. Shifts in color or muscle tone. Signs of activation going up or coming down. I'm pacing the work to stay inside your window of tolerance — enough activation to work with, not so much that you flood.
We might work with movement — a gesture, a postural shift, an impulse in the body. We might do something with breath. We might work with a part of you that's been carrying something for a long time and hasn't had the chance to say what it needs.
And then we close. That part matters. Sessions close with enough time to settle — to bring the activation down to baseline, to integrate what happened, to leave grounded. You don't leave raw. This is why 60 minutes, with additional time for grounding as needed, matters: the completion cycle needs to happen within the session.
For a science-based explanation of what somatic therapy is and how it works, read: What Is Somatic Therapy?
Anxiety Therapy Hollywood| Anxiety Therapy Raleigh| Somatic Therapy North Carolina

9. Nervous system regulation practices that actually do something
Let me be honest with you here, because there's a lot of advice about nervous system regulation on the internet and a lot of it ranges from mildly useful to effectively useless for people with chronic dysregulation.
Deep breathing videos. Gratitude journaling. "Grounding exercises" that involve naming five things you can see. Cold showers. Meditation apps.
These things are not nothing. For mild, situational stress, some of them are genuinely useful. But for a nervous system that has been in chronic activation for years — that has learned hypervigilance as its baseline, that has stored years of unresolved stress responses — these tools are like putting a band-aid over something that needs surgery. They manage the surface. They don't address the root.
That said, there are practices that work at the level of the nervous system rather than just the surface, and that you can start using outside of therapy. Here's what I actually stand behind:
Extended exhale breathing
The research on this is solid. A longer exhale relative to the inhale activates the parasympathetic nervous system — specifically the vagus nerve, which is the primary pathway for the ventral vagal state. The ratio matters more than the specific count: try inhaling for four counts and exhaling for six to eight.
What makes this different from generic deep breathing: you're not forcing deep breaths (which can actually increase anxiety by signaling that something is wrong). You're lengthening the exhale specifically. Slow, easy, natural inhale. Extended, relaxed exhale. Two to five minutes.
This works because it's directly stimulating the physiological mechanism of the parasympathetic response. Your nervous system can't fully distinguish between the extended exhale of genuine safety and the extended exhale you're creating deliberately.
Shaking
Animals do this naturally after a stress response — they shake, tremble, and discharge the mobilized energy before returning to baseline. Humans largely suppress this because trembling looks like weakness or loss of control.
Deliberate shaking — literally shaking your hands, your arms, letting your knees bounce, shaking out your whole body — can help discharge sympathetic activation. It feels strange and a little undignified. It works.
Orienting
This is one of the most underrated nervous system practices and it's completely free and takes about 30 seconds.
When you're activated, your vision narrows — literally. Tunnel vision is part of the threat response. Orienting deliberately counteracts this.
Slowly scan the room you're in. Let your eyes move without urgency. Take in the periphery. Let your gaze settle on something neutral — a plant, a patch of light, the texture of a wall. Notice that you can see the full room. Notice that there's no immediate threat in your visual field.
This sounds almost insultingly simple. It works because it's giving your nervous system direct perceptual data — not reassuring thoughts, but actual sensory information — that the environment is safe. The neuroceptive scan picks up this information and it can shift the state.
Moving your body —
But specifically in a way that completes the impulse
This is different from general exercise advice. When you're activated — anxious, wired, overwhelmed — your body has mobilized for movement. Fighting, running, pushing away. The sympathetic activation has a physical direction built into it.
Exercise helps because movement discharges sympathetic energy. But there's an additional layer: if you can move in a way that completes the impulse your nervous system activated — pushing against a wall when the impulse is to push something away, walking or running when the impulse is flight, any kind of vigorous movement when the impulse is fight — the completion is more complete.
The honest caveat
These practices are genuinely useful, and I don't want to undersell them. Regular use, especially the orienting and extended exhale practices, can meaningfully shift your baseline over time.
But here's what they can't do: they can't complete unresolved stress responses that have been stored for years. They can't widen a window of tolerance that narrowed in childhood. They can't process the accumulated activation of a nervous system that has been in chronic dysregulation. They are maintenance practices — important and worth doing — but not a substitute for the therapeutic work.
If you've been doing all the regulation practices faithfully and still feel chronically anxious, that's not a failure of the practices. It's a signal that you need something that operates at a deeper level.
10. When to get professional support — and what to actually look for
There's no bright line between "manageable with self-practice" and "needs professional support." But here are the signs that the nervous system work you need is beyond what self-regulation practices can provide:
Your anxiety has been present consistently for more than a year, regardless of life circumstances. The baseline level of activation doesn't change much even during low-stress periods. Your window of tolerance is narrow enough that moderate stress regularly tips you into overwhelm or shutdown. You've tried talk therapy and understood a lot but the anxiety hasn't shifted in the body. Rest doesn't restore you. The patterns are affecting your relationships, your work, or your sense of yourself in ways that concern you.
Any one of those is a reason to consider somatic therapy specifically. All of them together is a very clear signal. For California clients, somatic therapy is available entirely virtually through online therapy in Los Angeles and across California.
What to look for in a somatic therapist
Not everyone who uses the word "somatic" is trained in the same thing. Here's what I'd look for:
Specific training — Somatic Experiencing certification, training through The Embody Lab, Sensorimotor Psychotherapy training, or similar. The word "somatic" on a Psychology Today profile is not sufficient.
Experience with your specific presentation. A somatic therapist who primarily works with acute trauma may work very differently than one who specializes in chronic anxiety and nervous system dysregulation. Ask what they see most in their practice.
Session length. Somatic work is very hard to do effectively in 50 minutes. If a therapist offers somatic therapy in standard 50-minute insurance sessions, that's worth asking about. The work requires time.
Their own regulation. This is harder to assess from a website, but you can often feel it in a consult call. A dysregulated therapist cannot provide the co-regulatory resource that somatic work depends on. Trust your nervous system's read on the person.
Transparency about the approach. A good somatic therapist should be able to explain clearly what they do, why, and what the evidence base looks like. Vagueness or over-mystification is a yellow flag.
NC clients: anxiety therapy in Raleigh, Durham, Chapel Hill, and Charlotte are all available virtually. LA clients: anxiety therapy in Hollywood.LGBTQ+ clients:LGBTQ+ Affirming Therapy NC
11. Frequently Asked Questions
-
The autonomic nervous system is the primary biological driver of anxiety. It continuously assesses threat and safety, and generates the physiological responses — elevated heart rate, shallow breathing, muscle tension, cortisol release — that we experience as anxiety. Anxiety is not primarily a thought problem; it's a nervous system state. Thoughts are often the downstream effect of that state, not the cause.
-
Yes. Nervous system dysregulation is a learned physiological pattern, not a permanent condition. The nervous system retains neuroplasticity throughout life — the capacity to form new patterns in response to new experience. With consistent, appropriate intervention — somatic therapy, co-regulation, trauma processing, and regular regulation practices — the nervous system can learn new defaults. Full remission from chronic anxiety is achievable and happens regularly in somatic therapy.
-
It depends significantly on history, consistency, and the complexity of what's being addressed. For most people working somatically: noticeable shifts within 90 days, meaningful change in 2–6 months, and more durable reorganization over 6–18 months of consistent work. This is not a slow process relative to the years the patterns have been building — and 75-minute sessions accelerate it meaningfully compared to standard 50-minute therapy.
-
Yes. The theoretical foundations — Polyvagal Theory, Somatic Experiencing, trauma neuroscience — are grounded in peer-reviewed research. Multiple randomized controlled trials have examined somatic approaches to anxiety and PTSD with significant results. Meta-analyses of body-oriented psychotherapies show moderate-to-large effect sizes for anxiety and trauma presentations. The neuroscience underlying somatic approaches — including van der Kolk's research on subcortical trauma encoding — is published in leading academic journals and is increasingly mainstream in trauma treatment.
-
Mindfulness involves deliberately attending to present-moment experience, including body sensations, with nonjudgmental awareness. It's valuable and builds a skill that supports regulation. Somatic therapy goes further — it's actively intervening with the nervous system's physiological state, not only observing it. We're working with activation, titration, pendulation, and the completion of stress responses. Mindfulness can support the work; it's not a substitute for it for chronic dysregulation.
-
This is extremely common and has a specific explanation. For nervous systems that learned that vigilance was required for safety, dropping into relaxation can feel threatening. The lowering of the guard activates the threat response. Relaxation itself becomes a cue for danger. This is sometimes called "relaxation-induced anxiety" and it's one of the clearest signs that the dysregulation is deep enough to need somatic intervention rather than just relaxation practices. A skilled somatic therapist will know how to work with this response rather than push through it.
-
For many people, yes. What "going away" actually means: anxiety is no longer the default state. It appears proportionate to actual circumstances. It resolves after the threat has passed rather than lingering. The baseline level of nervous system activation is genuinely low rather than chronically elevated. Many of my clients describe full remission — not the absence of all emotion or stress, but the absence of anxiety as a constant companion. The nervous system can learn safety as its default just as thoroughly as it once learned threat.
You made it to the end of a GIANT guide on your nervous system.
That's not nothing. Most people don't read this far unless something in here landed — unless some part of this felt less like information and more like recognition.
If that's where you are: the free consult call exists for exactly this moment. It's 15 minutes, by phone, and it costs nothing. We'll talk about what's bringing you to this point, what you've already tried, and whether the work I do is the right fit for where you are.
If it's not the right fit, I'll tell you honestly and point you somewhere that is. That's the whole offer.
About the author
Katie Hargreaves, LCSW, LCAS, is a somatic therapist and nervous system specialist licensed in California and North Carolina. She has over 12 years in mental health and more than 4,000 therapy sessions, with training through Alchemy Somatics and The Embody Lab in Somatic Experiencing, polyvagal-informed approaches, breathwork, and Internal Family Systems. Her practice is LGBTQIA2S+ and BIPOC affirming. She sees clients online throughout North Carolina and in Hollywood, California.
Somatic Therapy in Hollywood, CA | Somatic Therapy NC | Anxiety Therapy NC | LGBTQ+ Affirming Therapy NC